-
-
Accueil -
Référentiels
-
Le Registre des méthodes et des outils pour la prise de décisions fondée sur des données probantes -
Méthodes et des outils en soutien au changement organisationne - Health Evidence™
- Échange de Synthèses
-
-
Formation
-
Outil de mesure des compétences en matière de prise de décision éclairée par des données probantes -
Évaluation des besoins en matière d’apprentissage pour la prise de décision éclairée par les données probantes -
Vidéos sur la compréhension des données probantes issues de la recherche -
Modules d'apprentissage en ligne -
Heures de bureau virtuelles en courtage de connaissances - Ateliers et webinaires
- Perfectionnement sur mesure de la main-d’œuvre
-
Mentorat d’impact pour le perfectionnement de la main-d’œuvre
-
-
Outils
-
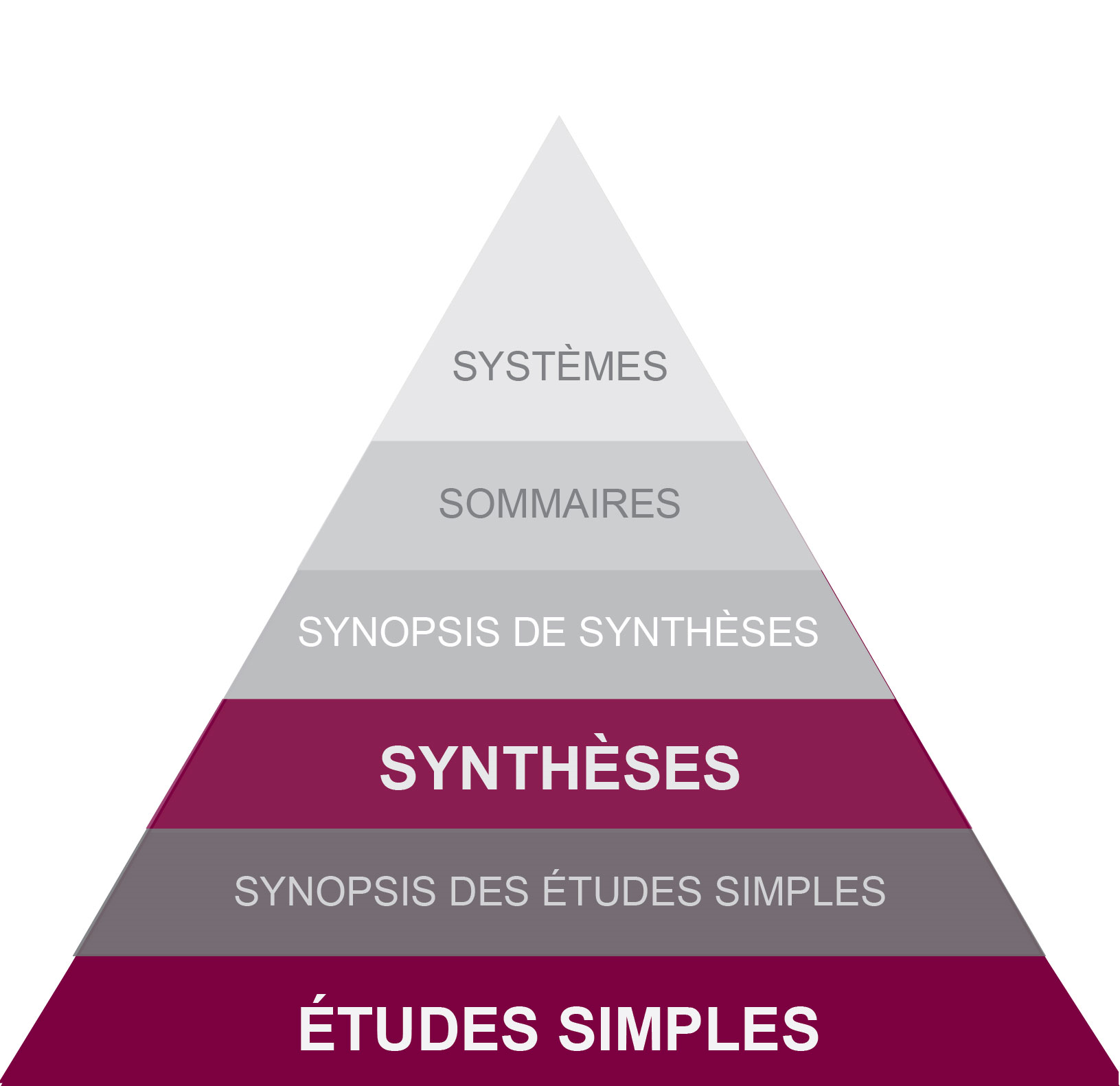
La Pyramide de recherche des 6 S -
Algorithme de classification des modèles d’études primaires -
Anatomie d'une revue systématique -
Outil d’évaluation de l’applicabilité et de la transférabilité des données probantes -
Outil de cartographie des compétences -
Prise de décision éclairée par des données probantes en santé publique -
EvSyS : l’outil de sélection des synthèses des données probantes à l’intention des décideurs -
Guide d’évaluation de la qualité des données probantes en santé publique -
Des ressources en santé mentale pour les travailleurs de la santé -
Outils d’évaluation de la qualité des données probantes issues de la communauté (ÉQDPIC) -
Guide pour les revues rapides -
Outil de planification et d’évaluation des ressources (PÉR)
-
- Service rapide de données probantes
-
Impact
-
Recueil sur la prise de décisions fondée sur des données probantes -
Résultats du Programme de mentorat en courtage de connaissances -
Pourquoi ça compte -
Publications du CCNMO -
Témoignages d'utilisateurs -
Relations externes -
Bourses d’application des connaissances
-
-
À propos de nous
-
Au sujet du CCNMO -
Notre bailleur de fonds -
Notre établissement d’accueil -
Les centres de collaboration nationale -
Membres de l'équipe -
Le comité consultatif -
Étudiants - COVID-19 Evidence Network to support Decision-making (COVID-END)
-
Communiquez avec nous
-
-